Workplace first aid in Indonesia goes by the acronym P3K. Full name: Pertolongan Pertama pada Kecelakaan. It’s regulated under Permenaker No. PER.15/MEN/VIII/2008, which most safety officers just call Permenaker 15/2008. That’s where any conversation about Indonesian workplace first aid has to start.
Below: what the regulation actually requires, what gets taught in standard P3K courses, and where VR-based training fits or doesn’t.
What Permenaker 15/2008 puts on employers
Four obligations.
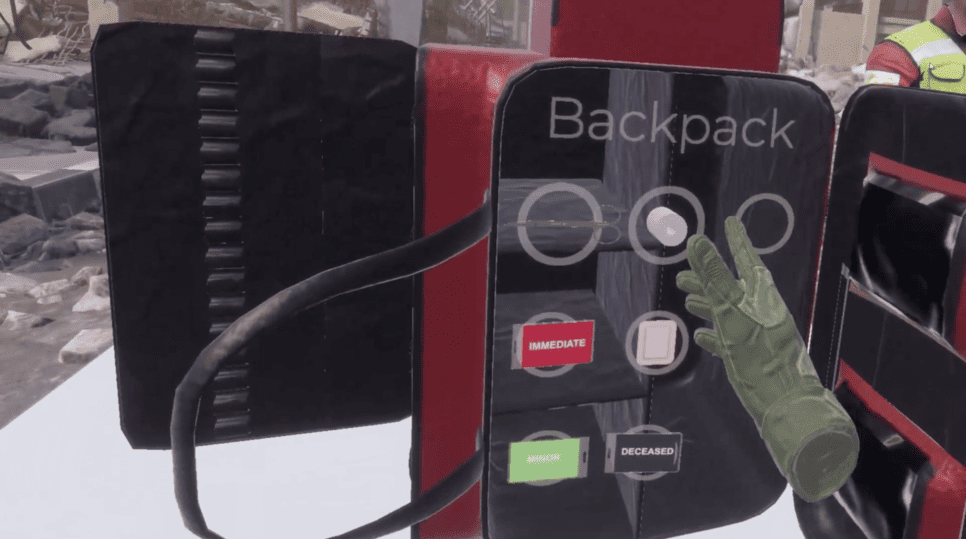
Provide first aid services in the workplace. Appoint Petugas P3K, with the minimum count tied to workforce size and risk classification (low-risk versus high-risk, defined in the articles). License each Petugas P3K through the Director General of Manpower Inspection or an appointed official, after accredited training. Equip the workplace with a P3K kit (kotak P3K) whose minimum contents are listed in the appendix, plus a P3K room once size or risk thresholds are crossed.
The regulation is methodology-neutral. It tells you what outcome to produce. It doesn’t tell you how to get there.
It also doesn’t lock in a mandatory refresh interval in the text itself, though most certifying bodies recommend recertifying every two to three years. Healthcare facilities, mining, oil and gas all carry sector-specific rules on top. Permenaker 15/2008 stays the baseline.

What standard P3K courses cover
Accredited P3K training in Indonesia comes through PMI, BNSP-recognized providers, or licensed instructors aligned with PERKI references. Basic certification runs 16 to 24 hours over two to three days. The curriculum is stable across providers.
It covers CPR and AED use. Bleeding control, wound care, burns (thermal, chemical, electrical). Fractures and immobilization. Sprains and soft tissue injuries. Shock recognition. Eye and ear injuries. Heat illness, cold illness. Choking across age groups. Poisoning and chemical exposure. Patient transport, handover, documentation.
That’s wide ground for 16 to 24 hours. Each topic gets touched. None gets drilled deep. That’s just the math of a short certification course, and it’s not really fixable inside the course itself.
The procedures, briefly stated
Indonesian P3K courses teach the same procedures everyone else does. CPR and BLS follow American Heart Association guidance, with PERKI references for the national overlay. Trauma and medical emergency response uses standard first aid protocol that crosses most national programs.
A few anchors worth stating directly.
Scene check before patient contact. No live electrical, no fire, no traffic, no structural risk, no chemical release. This step heads every framework for a reason.
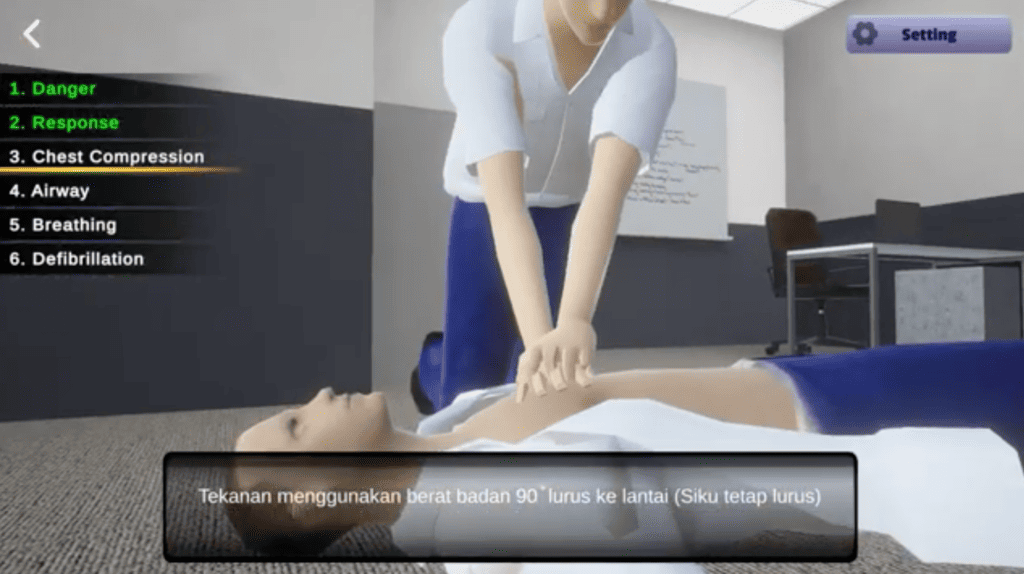
Primary survey runs DRSABCD: Danger, Response, Send for help, Airway, Breathing, CPR, Defibrillation. Each step before the next, no skipping ahead.
Adult CPR is 100 to 120 compressions per minute, 5 to 6 cm depth, 30:2 with rescue breaths for trained responders. Compressions-only is fine when rescue breathing isn’t possible.
External bleeding: direct pressure first. Pressure dressing if that’s not enough. Tourniquet only for severe limb hemorrhage pressure can’t control. (Tourniquet protocols have shifted over the past decade in line with current trauma evidence.)
Thermal burns get cool running water for at least 20 minutes, then a non-adherent dressing. No ice. No butter. No toothpaste. No topical home remedies, period. Chemical burns flush with copious water, with substance-specific protocols where they apply.
Suspected fractures get immobilized in the position found. Splinting uses available rigid material, padded, secured firmly enough to prevent movement but not tight enough to cut off circulation.
Choking: back blows alternated with abdominal thrusts (Heimlich) for adults and conscious children. Back blows alternated with chest thrusts for infants. If the victim loses consciousness, transition to CPR.
Recovery position for breathing-but-unresponsive victims, except where spinal injury is suspected.
These procedures are simple to describe. Doing them correctly in real time, with a real victim, on an active scene, is the harder problem. That gap is what training methodology actually has to close.
Skill decay is the real problem
First aid skills decay without practice. AHA and ERC guidance both reference this directly, and the underlying literature is consistent enough to treat as a planning input rather than a research debate.
The pattern looks like this. Compression depth and rate (the most measurable parts) start declining within three to six months. By twelve months without practice, performance can drop substantially, and on some specific competencies it approaches pre-training baselines. Cognitive knowledge holds up better than tactile skill. Frequent short refreshers retain skills better than infrequent long courses.
What this means for workplace P3K is straightforward. Annual recertification is enough to keep regulation happy. It’s not enough to keep skills functional through the eleven months between certifications. Whether that’s a problem depends on the operation. Low-risk office, regulatory minimum is probably fine. Higher-risk industry, or any operation that wants its Petugas P3K to actually function when it counts, you need more practice frequency than annual courses provide.
That’s the operational gap VR was built to address.
Where VR fits, and where it doesn’t
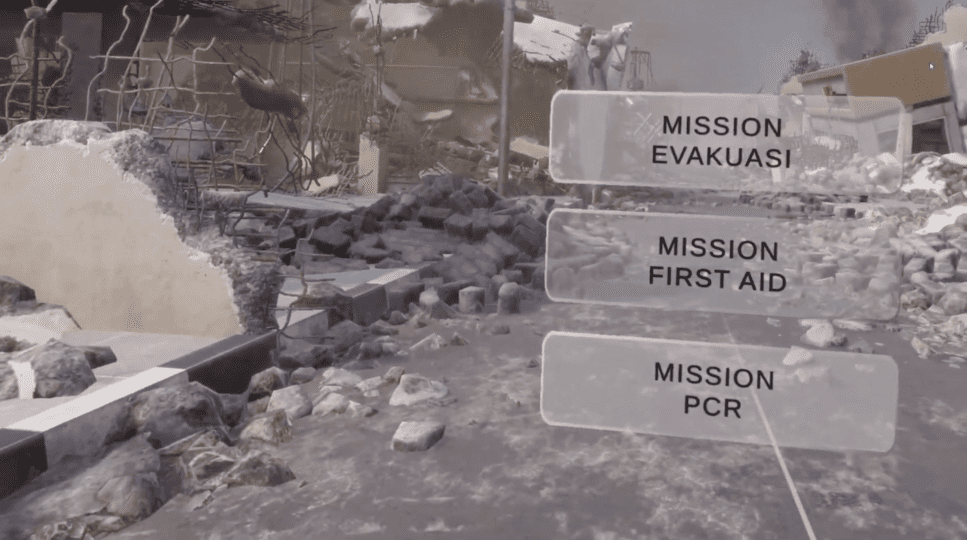
VR training puts the user in a 3D simulated environment, head-mounted display, motion controllers. The system runs a scenario, tracks user actions, feeds back against protocol.
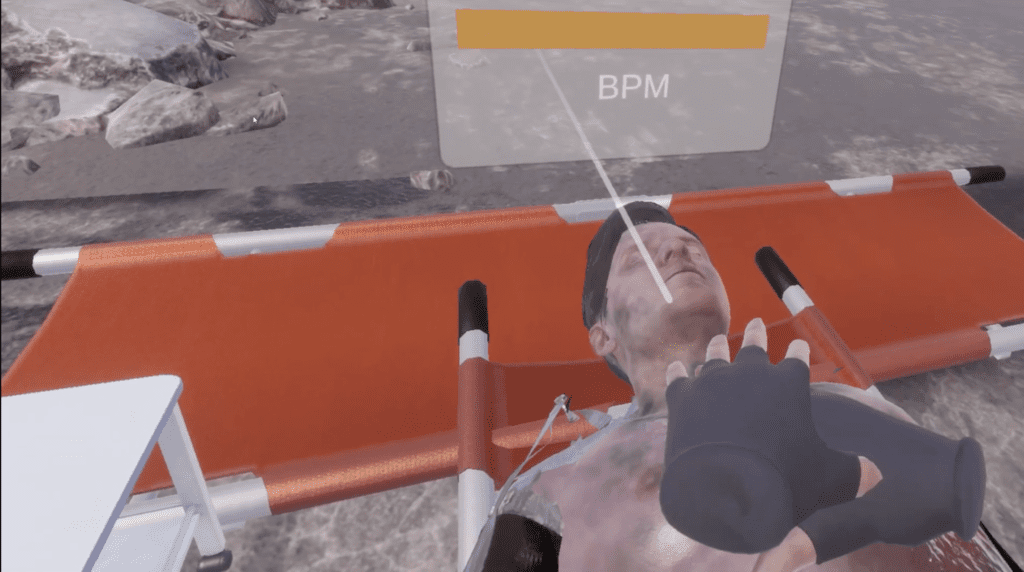
What VR adds is practice frequency at a unit cost conventional training can’t match. Sessions run 8 to 15 minutes. No instructor coordination required. Multiple scenarios per session. For procedures with measurable parameters (CPR rate and depth, mostly) the system logs performance per session, which gives you competency telemetry instead of a single binary pass-fail. That matters during K3 audits, where attendance records are weak evidence and trend data isn’t.
What VR doesn’t do is replace accredited certification. A Petugas P3K licensed under Permenaker 15/2008 is licensed through accredited courses, not VR. VR sits between certifications, not in place of them. It also doesn’t replace tactile practice. Pressure dressing, splinting, Heimlich, these still need physical handling on a manikin or partner. Controller haptics aren’t the same thing as a real chest, a real limb, or a real airway.
Cleaner way to frame it: accredited courses cover certification, physical manikins cover tactile skill, VR covers practice frequency between cycles. Each tool covers something the other two can’t, and using all three is what a serious P3K program actually looks like.
VGLANT specifics
VGLANT is built by PT Virtu Digital Kusuma, an Indonesian AR, VR, MR, and Digital Twin company headquartered in Jakarta with engineering in Bandung. The first aid module covers the standard P3K scope: CPR, AED use, bleeding control, burns, fractures, choking, shock.
UI and voice prompts default to Bahasa Indonesia, with English available for multinational deployments. Protocols align with AHA BLS guidance and PERKI references for resuscitation, plus standard first aid protocol for trauma response. Hardware runs on standalone headsets, currently IDR 7 to 25 million per unit depending on consumer-grade Meta Quest 3 or enterprise-tier with managed software. Content licensing is separate, per-seat or per-site annually.
The first aid module shares hardware with the rest of VGLANT’s K3 catalog, including fire response, APAR operation, hazardous material handling, and confined space. An organization buying VR for one use case extends across the rest of the catalog without additional hardware spend, which matters during procurement when finance asks why the headsets exist.
For specifications or pilot scoping, contact enquiry@vglant.com or +62 818 0755 5538.