Most companies that approach about VR-based CPR training are looking for the same thing. They want a way to keep P3K personnel sharp between certification cycles without the cost and disruption of repeating full classroom courses every quarter. That’s a reasonable problem to solve. Whether VR is the right answer depends on workforce size, site distribution, and how seriously the organization treats skill retention as a measurable outcome.
This piece is meant as a working reference for HSE and HR teams evaluating the technology, not a sales pitch.

The regulation, briefly
Permenaker No. 15 Tahun 2008 sets the rules for workplace P3K (Pertolongan Pertama pada Kecelakaan) in Indonesia. It specifies how many trained first-aiders an employer must maintain, based on headcount and risk classification. It does not specify how to train them, and it does not specify any meaningful refresh interval. Methodology is left to the employer.
In practice, most companies translate this into one annual session run by PMI, an in-house safety officer, or a private provider. Certificate signed, file closed, audit passed. Whether anyone in that room can actually do CPR six months later is a separate question, and almost no internal audit ever asks it.
Cardiac arrest, and why bystanders matter more than ambulances
Cardiac arrest is when the heart’s electrical system fails and circulation stops. It is not a heart attack, though the two get confused often enough that this distinction matters even at the awareness level. A heart attack is a blocked artery, and the victim is usually conscious. Cardiac arrest drops a person where they stand. From that moment, every minute without compressions costs roughly 10 percent of survival probability. Brain injury starts around the four-minute mark.
Now look at ambulance response in Indonesia. Jakarta and Surabaya during peak traffic, you’re realistically looking at 8 to 15 minutes. Bekasi and Tangerang, often longer. Industrial sites in Cilegon, Cikarang, and Karawang frequently push past 20 minutes once you factor in gate clearance and access roads. The implication is straightforward. Whoever is standing next to the victim is the one who decides the outcome, and that person is, statistically, not a doctor.
Why annual classroom training underperforms
Skill decay in first-aid contexts is well documented. Resuscitation Council UK and the American Heart Association both publish on it. The consistent finding is that hands-on procedural skills, particularly compression depth, compression rate, and AED operation, start measurably degrading within three months of training. By the twelve-month mark, retention is poor enough that bystanders trained a year ago tend to perform closer to untrained controls than to fresh trainees.
This is not an indictment of conventional training. It’s an indictment of training frequency. Annual sessions don’t fail because the content is bad. They fail because muscle memory doesn’t survive twelve months of disuse. The fix isn’t a better instructor. It’s more reps, which is exactly the thing in-person training makes expensive and impractical to deliver at scale.
What VR actually does differently
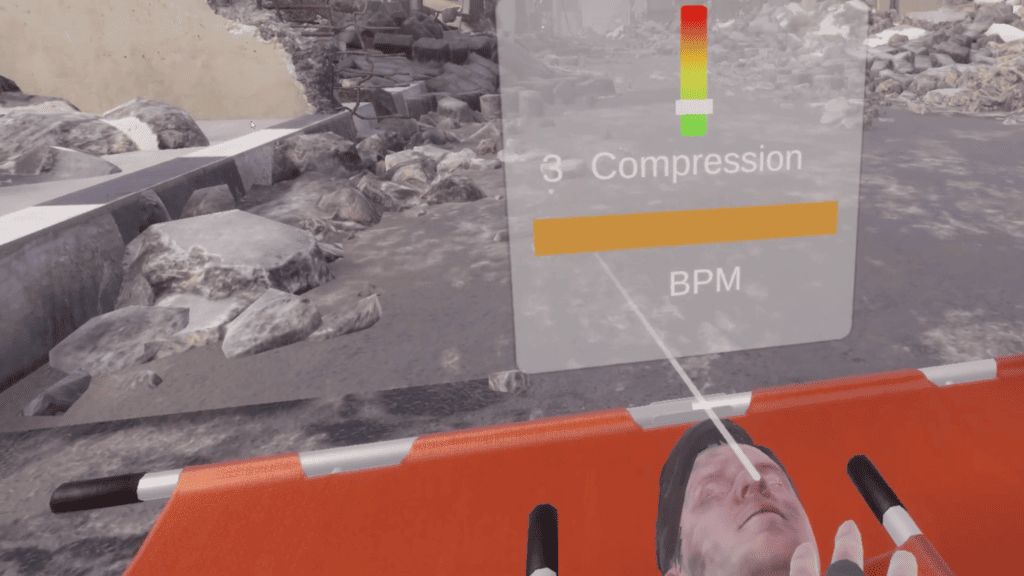
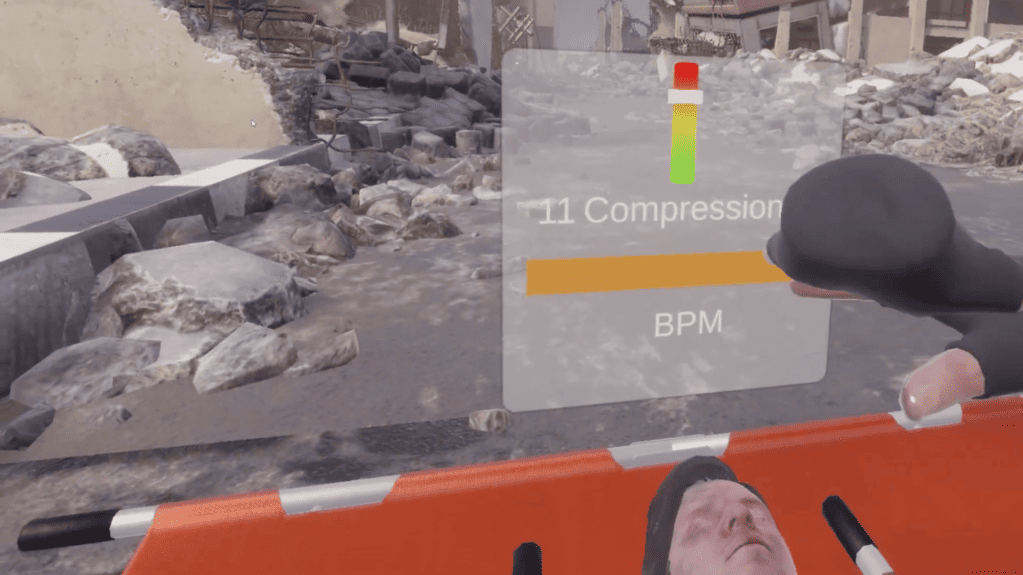
A VR CPR module runs on a head-mounted display. In current Indonesian deployments, that’s typically a Meta Quest 3 or a Pico 4. The trainee puts on the headset, picks up the controllers, and walks through the full protocol in a simulated environment. The system tracks compression rate and depth through controller position data, gives real-time feedback when the rhythm drifts, and scores the session.
The procedural content itself is the same as what PMI or an AHA-aligned provider teaches in person. Hazard check before approaching. Responsiveness verification. Calling 119 and assigning a specific bystander to fetch the AED. Airway and breathing assessment. Compressions at 100 to 120 per minute, 5 to 6 cm depth. AED pad placement, rhythm analysis, shock, resume.
What changes is the practice loop. In-person training typically gives an employee 5 to 10 minutes on a manikin once a year. VR lets them run the full sequence in roughly 8 to 12 minutes whenever they have the time. Monthly is not unreasonable. That’s the mechanism that keeps the skill from rotting between certifications.
Studies on VR-based procedural training in healthcare and emergency response, including work published in JMIR Serious Games and Resuscitation, generally report better skill retention than classroom-only methods. Effect sizes vary depending on which protocol step is being measured. The effect is real but modest at the individual session level. The larger operational win is being able to repeat sessions cheaply, often, and on the trainee’s schedule rather than the instructor’s.

Where VR fits, and where it doesn’t
VR does not certify anyone. Indonesian employers required to maintain certified P3K personnel still need accredited courses, whether through PMI, BNSP-recognized providers, or licensed BLS instructors. VR sits between certifications, not in place of them.
It is also not a substitute for hands-on practice on a real manikin. The haptic feedback from a controller is not the same physical sensation as compressing an actual chest. Most serious deployments combine the two. Headset for protocol drilling, decision-making under simulated pressure, and refresher cycles. Physical manikin for compression mechanics.
Where VR pays for itself:
- Multi-site organizations where flying instructors around is operationally painful
- Workforces with rotating shifts where scheduling group sessions is constant friction
- Industries with elevated cardiac risk profiles, including oil and gas, manufacturing with older workforces, and security services covering large facilities
- Organizations that need measurable competency data for K3 audits, not just attendance records
Where it probably isn’t worth it:
- Single-site offices under 100 people with stable staffing and a strong existing PMI relationship
- Organizations whose actual problem is that nobody is certified at all. Fix that first.
VGLANT specifications
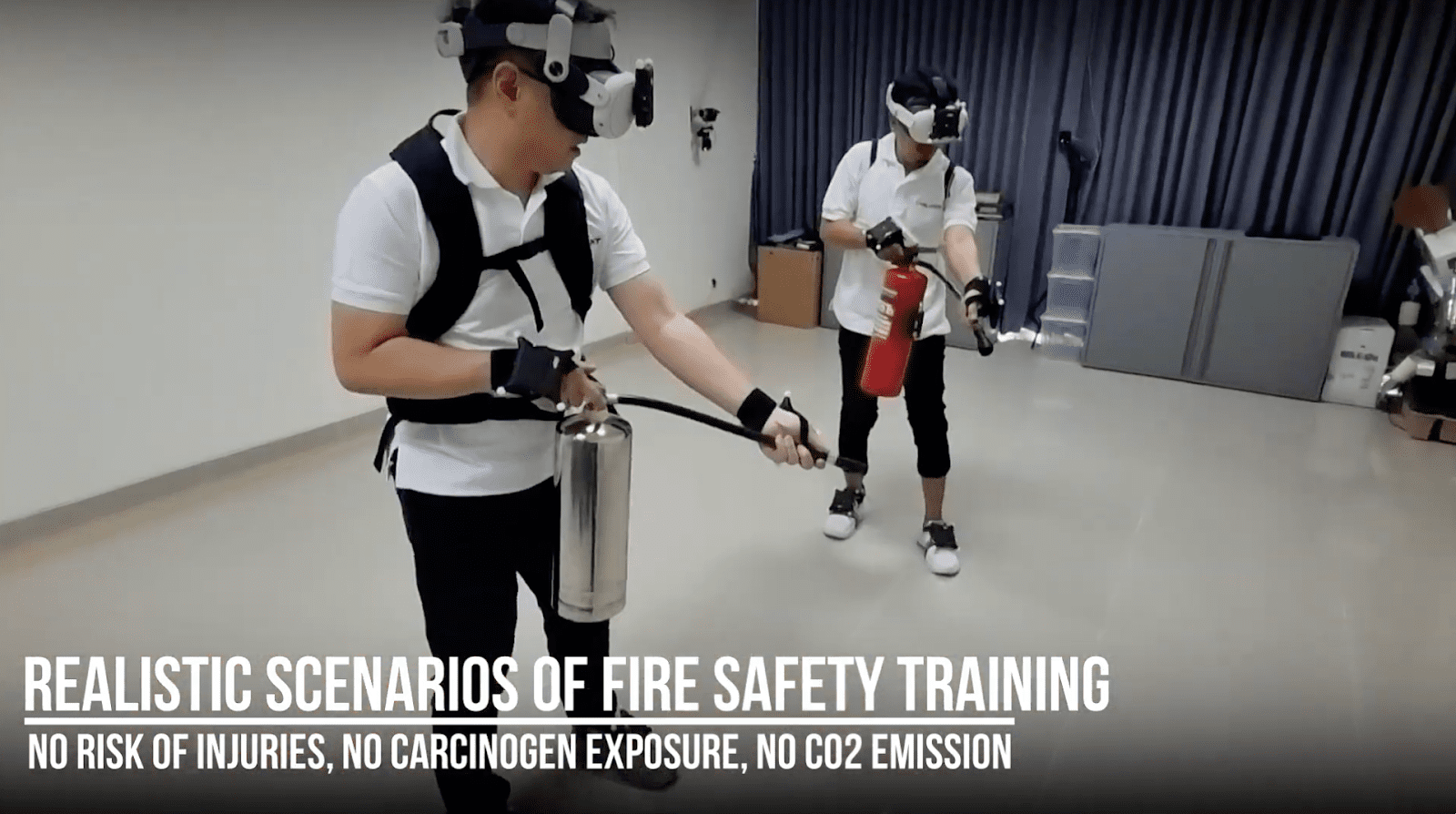
VGLANT is built by PT Virtu Digital Kusuma, an Indonesian AR, VR, MR, and Digital Twin firm with offices in Jakarta and Bandung. The CPR module sits within a broader catalog that also covers fire safety, APAR operation, hazardous material handling, and confined space scenarios. Practically, this means the same headset and the same platform run multiple K3 training programs, which matters during procurement when finance asks why you’re buying VR hardware for one use case.
A few things worth flagging.
Voice prompts and on-screen UI come in Bahasa Indonesia by default, with English available for multinational sites. Scenarios are modeled on Indonesian workplace environments rather than generic Western office layouts, which sounds cosmetic until you watch a trainee in a Cikarang factory hesitate because the on-screen fire extinguisher signage doesn’t match what they actually see at work. Protocols are aligned with AHA BLS guidelines and Permenaker P3K requirements. Local support handles deployment, pilot facilitation, and on-site troubleshooting in the same timezone, which sounds minor until you’ve tried resolving a firmware issue with a US-based vendor at 3 AM Jakarta time.
Cost realities
Headset hardware in current Indonesian pricing runs roughly IDR 7 million to IDR 25 million per unit, depending on whether you’re buying consumer-grade Meta Quest 3 hardware or enterprise-tier devices with management software bundled in. Content licensing is separate, usually on per-seat or per-site annual terms.
For a 200-person manufacturing operation on a single site, breakeven against conventional annual training typically lands somewhere between year two and year three. For a 1,000-plus headcount organization spread across multiple sites, it’s usually faster, sometimes within the first year if they were already paying significant amounts for in-person delivery. The math tilts further toward VR when the organization wants to run monthly or quarterly refreshers, because that’s the scenario where conventional training becomes financially impractical regardless of intent.
A pilot of 5 to 10 headsets, run for two to three months on a single site, is the standard route to validate fit before wider rollout. That’s the path most VGLANT clients take, and it’s the right one. Buying 50 headsets up front for a use case nobody has tested at your specific site is how procurement decisions go sideways.
What to nail down before signing
A few items worth pinning down with any VR training vendor, not just VGLANT, before procurement.
Whether the protocols match your existing certification body. AHA, ERC, and Australian Resuscitation Council protocols differ in small but real ways. If your certifying provider follows AHA, your VR content should too, otherwise you’re training two slightly different procedures and trainees notice.
How the session data integrates with your LMS. Most enterprise organizations want competency records living in the same system as the rest of training, not in a separate vendor portal that nobody opens after the first quarter.
Sanitation and rotation logistics. Headsets get shared. Plan for face cushion replacement, surface wipes, and storage that doesn’t kill battery life. This is unglamorous but it’s where deployments quietly fail.
Where content is hosted and who owns the session data. Indonesian data residency requirements apply to some sectors and not others, and it’s worth getting clarity early rather than negotiating it after the fact.
For technical specifications, pilot scoping, or a platform walkthrough, VGLANT can be reached at enquiry@vglant.com or +62 818 0755 5538.